
The main things to watch at night
- Most healthy adults breathe in the same broad range as awake rest, often a little lower once asleep.
- REM sleep makes breathing more irregular, so a changing rhythm is not automatically a problem.
- Repeated pauses, gasping, or loud snoring matter more than one slightly low number.
- Persistent fast or very shallow breathing can point to a sleep disorder or another medical issue.
- Home measurements are most useful when you track patterns across several nights, not one isolated reading.
How I interpret a normal respiratory rate while sleeping
There is no single sleep-only number that fits every healthy adult. As a practical rule, an awake resting rate of 12 to 20 breaths per minute is normal, and many people drift a little lower once asleep, often into the low-to-mid teens. What matters more than the raw count is whether the breathing stays smooth, deep enough, and free of repeated pauses.
| Situation | What is commonly seen | How I read it |
|---|---|---|
| Awake, resting adult | About 12 to 20 breaths per minute | Use as your baseline, not as a diagnosis |
| Typical sleep | Often slightly slower, especially in non-REM sleep | Usually normal if the pattern is steady and you feel well |
| REM sleep | More irregular, with small swings in pace | Normal variation, not automatically a disorder |
Children and infants breathe faster, so adult ranges should not be applied to them. Once you know the expected range, the next question is why the pattern changes across the night.
Why breathing changes across the night
Once sleep starts, breathing is controlled more by automatic brainstem signals and less by conscious effort. Muscle tone drops, oxygen demand eases a little, and the breathing pattern often settles into a quieter rhythm. That is why sleep usually looks calmer on paper than wakefulness does.
In non-REM sleep, breathing is usually the most regular. In REM sleep, the rhythm often becomes less predictable, even in healthy sleepers. I do not treat that as a problem by itself, because REM is meant to be a more variable stage. The key question is whether the variation is brief and expected, or whether it turns into recurring pauses, gasps, or obvious strain.
Body position, nasal congestion, alcohol, sedatives, and extra soft tissue around the airway can all make nighttime breathing less stable. That is why a good interpretation always includes the person’s sleep context, not just the number on a screen. That context becomes especially important when a rate is not just different, but clearly too slow, too fast, or repeatedly interrupted.
When a slower or faster rate starts to look abnormal
A lower rate during sleep is not automatically alarming. I start to worry when the pattern is persistently shallow, repeatedly interrupted, or paired with symptoms of low oxygen.
| Pattern | What it can suggest | Why it matters |
|---|---|---|
| Repeatedly very slow breathing, especially with shallow breaths | Bradypnea or hypoventilation | Carbon dioxide can rise and oxygen can fall |
| Repeatedly fast breathing, often above 20 to 25 breaths per minute at rest | Tachypnea, pain, fever, anxiety, lung or heart strain | The body may be working harder than it should |
| Breathing pauses of 10 seconds or more, followed by gasps or snorts | Apnea | This is a classic sleep-disordered breathing pattern |
| Dizziness, confusion, chest pain, blue lips, or severe shortness of breath | Possible oxygen problem | Needs urgent medical attention |
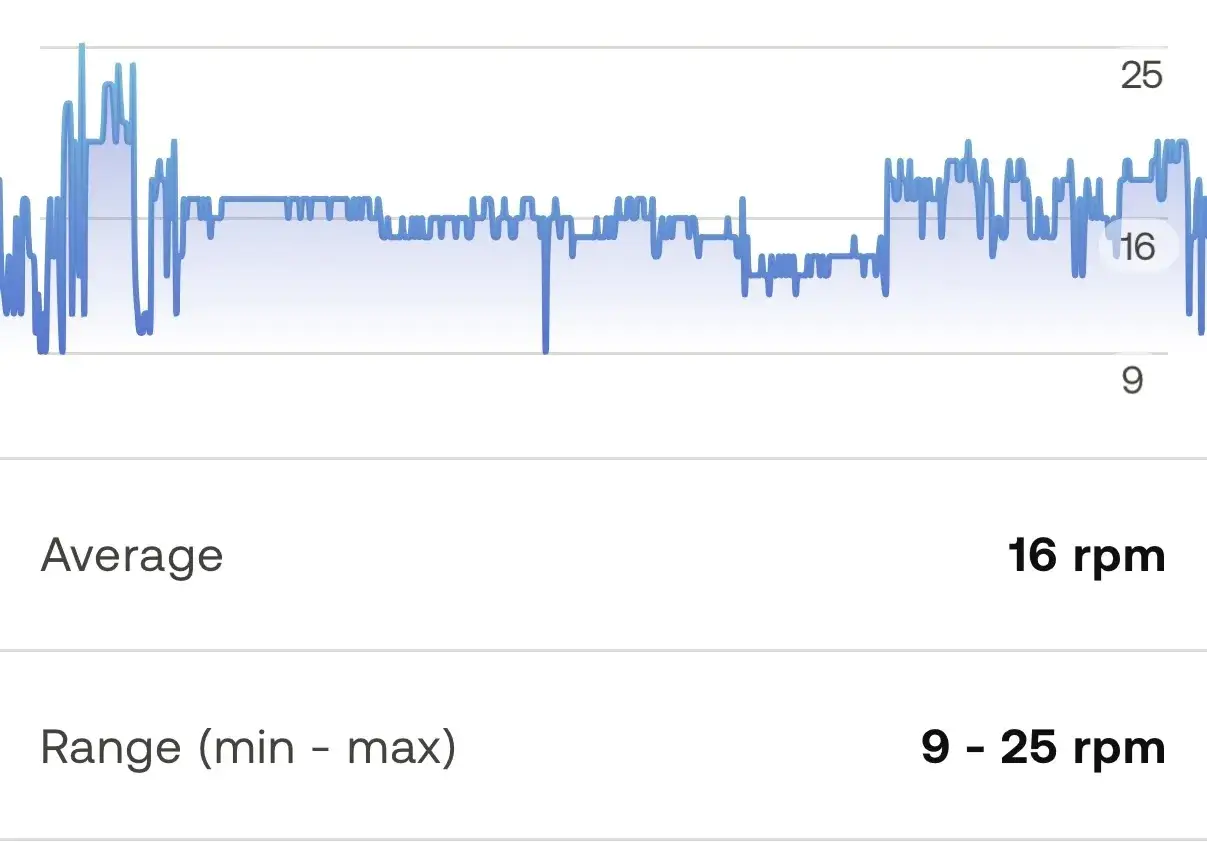
One detail many people miss: a person can have a normal average breathing rate and still have apnea events. The average hides the pauses, and the pauses are often the real problem. Those pauses are also what most often point toward a sleep disorder.
Sleep disorders most often linked to abnormal nighttime breathing
Normal snoring and sleep apnea are not the same thing, and not every breathing complaint points to the same cause. What matters is the pattern: blocked-airway pauses, absent breathing drive, or shallow overnight ventilation each point in a different direction.
| Sleep problem | Typical nighttime pattern | Common clues |
|---|---|---|
| Obstructive sleep apnea | Airway collapses, so breathing stops and restarts | Loud snoring, gasping, unrefreshing sleep, daytime sleepiness |
| Central sleep apnea | The brain does not send steady breathing signals | Repeated pauses without the usual snoring pattern; can be linked to certain medical conditions or opioid use |
| Obesity hypoventilation syndrome | Breathing is too shallow to clear carbon dioxide well | Morning headaches, daytime sleepiness, obesity, low energy |
| Simple snoring | Air moves through a narrowed airway but without clear pauses | Noise may be the main issue, though it can still coexist with apnea |
A normal breathing rate does not rule sleep apnea in or out. Sleep studies look beyond the rate itself, and in adults an apnea-hypopnea index below 5 events per hour is considered normal. That is why I never rely on breathing rate alone when I am trying to understand whether sleep is healthy or disrupted.
How to measure it at home without fooling yourself
If you want a useful home reading, the setup matters as much as the count. I would not measure breathing right after climbing stairs, talking, or scrolling in bed, because the number will reflect activity rather than sleep physiology.
- Lie still for at least 5 minutes before you count.
- Count one full minute, not 15 or 30 seconds.
- Use one inhale plus one exhale as one breath.
- Repeat the check on more than one night, because sleep position and congestion can change the result.
- Write down snoring, awakenings, alcohol use, sedatives, and whether you slept on your back or side.
Wearables can help spot trends, but I would not treat a ring or watch as a diagnostic device. Motion, loose fit, poor sensor contact, and sleep-stage estimation can all skew the number. The most useful data is a pattern over several nights, especially when it lines up with symptoms.
What bedroom habits can improve nighttime breathing
When the cause is positional or congestion-related, the bedroom itself can make a real difference. I focus on changes that reduce airway resistance without pretending they solve every breathing disorder.
- Sleep on your side if snoring or mild airway collapse is worse on your back.
- Raise your head slightly with a wedge or adjustable base if reflux, congestion, or postnasal drip is part of the problem.
- Keep the air comfortable and clean by managing dust, pet dander, and dryness.
- Avoid alcohol close to bedtime because it relaxes airway muscles and can worsen snoring and apnea.
- Treat nasal blockage with saline, allergy management, or clinician-guided care when congestion is chronic.
- Address weight-related risk if that is relevant, because extra soft tissue around the neck can narrow the airway.
These changes can help, but they are not a substitute for medical treatment if breathing stops, oxygen drops, or daytime sleepiness is becoming hard to ignore. That is the point where the next step is evaluation, not another pillow.
What I would do if the pattern keeps looking off
If the pattern is only a little slower than daytime and you wake up feeling fine, I would watch it rather than panic. If you are seeing repeated pauses, gasping, loud snoring, morning headaches, dry mouth, or daytime sleepiness, I would ask for a sleep evaluation. And if you have chest pain, blue lips, confusion, or severe shortness of breath, that is urgent.
In a clinic or sleep lab, the next question is usually not just how fast you are breathing. It is whether oxygen stays stable, whether airflow is blocked, and how many apnea or hypopnea events occur per hour. That is the data that separates a normal variation from a disorder worth treating.
My practical rule is simple: a lower rate at night is usually fine when the breathing is smooth, the sleep is restorative, and the symptoms are absent. Once the pattern becomes shallow, irregular, or disruptive, I treat it as a signal to look deeper.